
Education & Resources
Renal Physicians
about | home
| |
|
|
Education & Resources Renal Physicians |
communication | vision about | home |
Dear Nephrolors':
We recently had a discussion as to what to do when a fistula develops with aberrant
drainage down the arm instead of up. I thought everyone might like to see how this
can be used in revising the drainage in a fistula by interventional, non-surgical
techniques.
The patient presented with a painful shoulder. He had a left upper arm fistula which
was 6 months old. On exam the fistula was patent from the elbow to the middle of the
biceps. Above that was a hard cord for about
4 to 6 cm. and then nothing. pic #1 and #2 demonstrate the drainage as I first found it on
angiography. The arrows demonstrate the direction of flow. The flow went up
the arm to the level of the biceps (#1) and then turned 180 degrees south towards the
elbow. In #2 you see (follow the arrows) how the drainage went down to below the
antecubital fossa and then spread into multiple channels. The fistula was very
hyper-pulsatile clinically and I feared the whole access would clot if left alone. I
was able to get a wire around all of this and actually up to the central circulation and
therefore I felt we could potentially create a useable channel. #3 illustrates an 8 mm
balloon in the fistula over the wire. This photo demonstrates how tight some of the
strictures were (see the waists on the left half of the balloon). These areas were
present in pretty much the entire drainage. I am leaving out the majority of the technical
details. If anyone is interested I will be happy to provide them. The original
channel was so small (tight) that the wire and balloons occluded it to the point that
significant clot formed and flow stopped. #4 demonstrates the clot which shows up as
filling defects within the dark areas of contrast. I proceeded to occlude the
channel with a balloon inflated deep in the outflow and laid 1.25 mg of tPA throughout the
area of clot and manually "kneaded" the fistula. I also heparinized the
patient. #5 demonstrates the final result. Again the flow goes down to the
right below the elbow and then in a big circle up the basilic system to the central
circulation. Please note that the collateral channels that were seen on #2 have
disappeared. This was accomplished without ligating any vessels. Thus it
demonstrates my contention that if one simply dilates and creates a main channel, the flow
will go into it preferentially, making ligation often not necessary.
Let me know if you have questions. As always comments are welcome. I hope this
was enjoyable and educational.
Don
Donald Schon, MD, FACP
LifeLine Vascular Lab
Phoenix, AZ
(To View Original Image Click on Thumbnail)
 Image 1 |
 Image 2 |
 Image 3 |
 Image 4 |
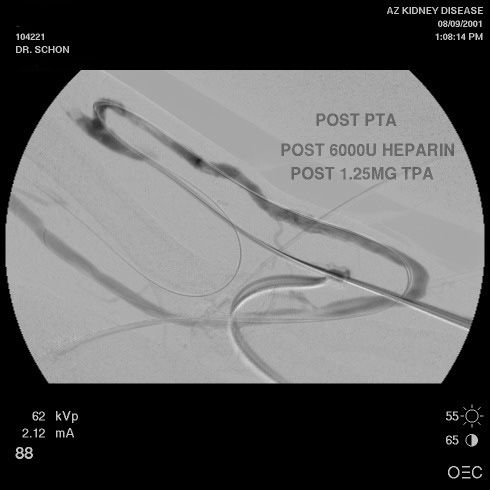 Image 5 |
| Copyright � 2000-2007 cyberNephrologyTM
All rights reserved. Last Modified: Thursday March 08, 2007 05:21:10 PM |
[email protected] |