
about | home
| |
|
|
|
education | vision about | home |
|
We have had a case of sudden graft loss after over 2 years post-transplant, with an unusual histology. I would be interested in your thoughts.
The clinical history is a 44 year old male, ESRD due to reflux nephropathy, first cadaveric renal transplant 1999 with good function. He recently had moderately severe hypertension, and ACE inhibitor therapy was started. On 3rd January 2002, he was seen at a clinic obviously unwell, with sudden loss of function, anuric, sCr had increased from 170 to 440umol/l and febrile. Perfusion scan showed renal artery occlusion. No biopsy was performed; he had a transplant nephrectomy the next day.
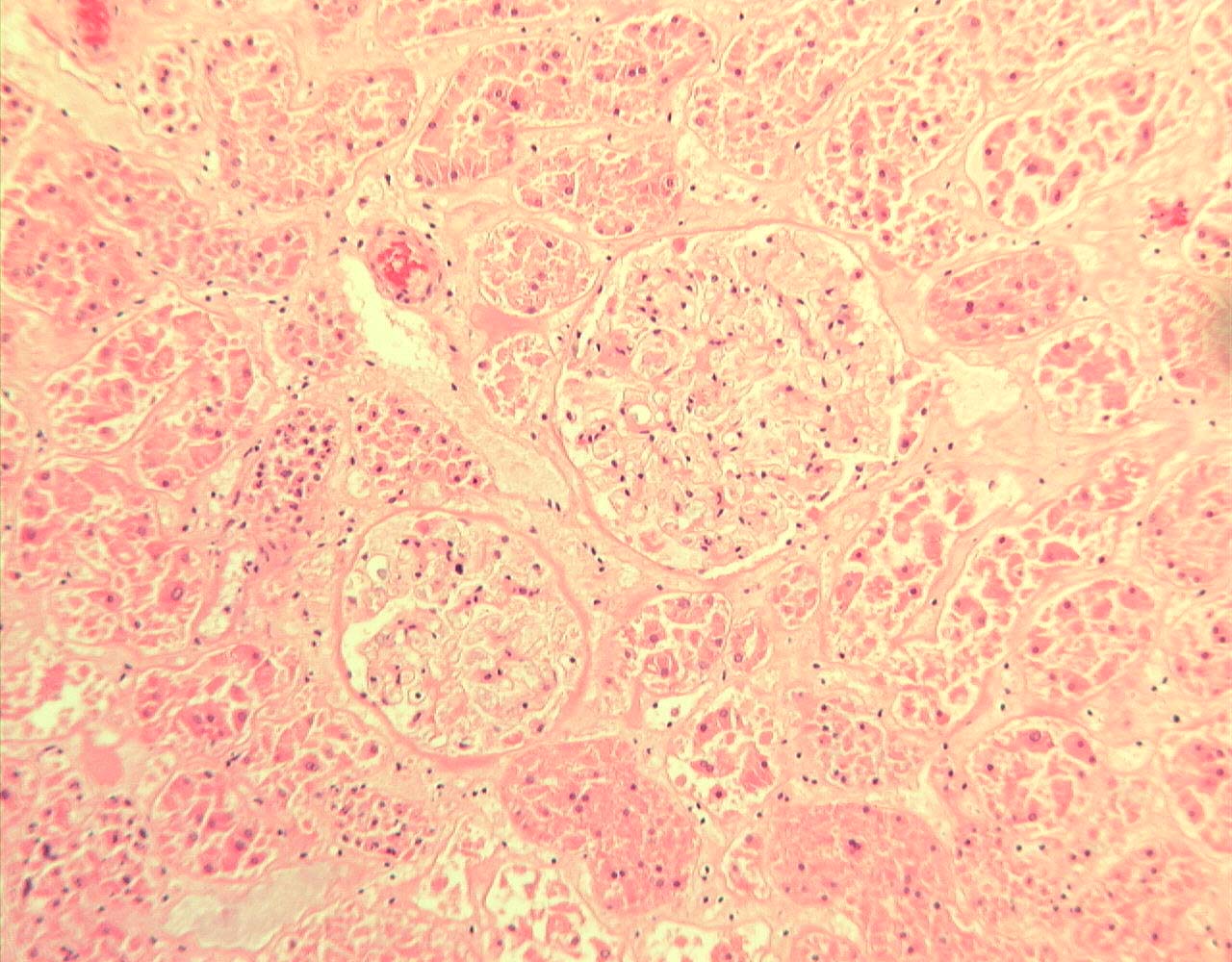
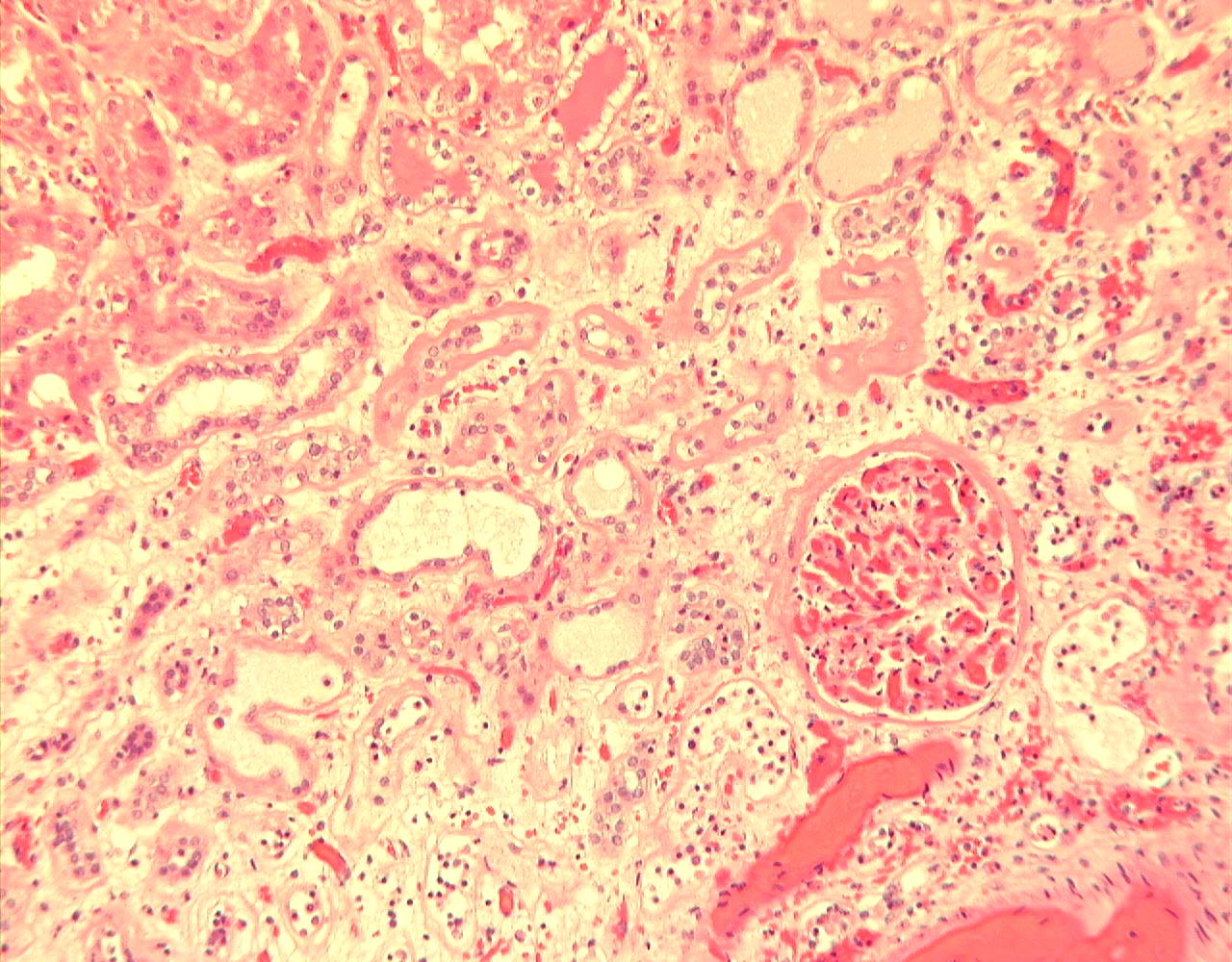
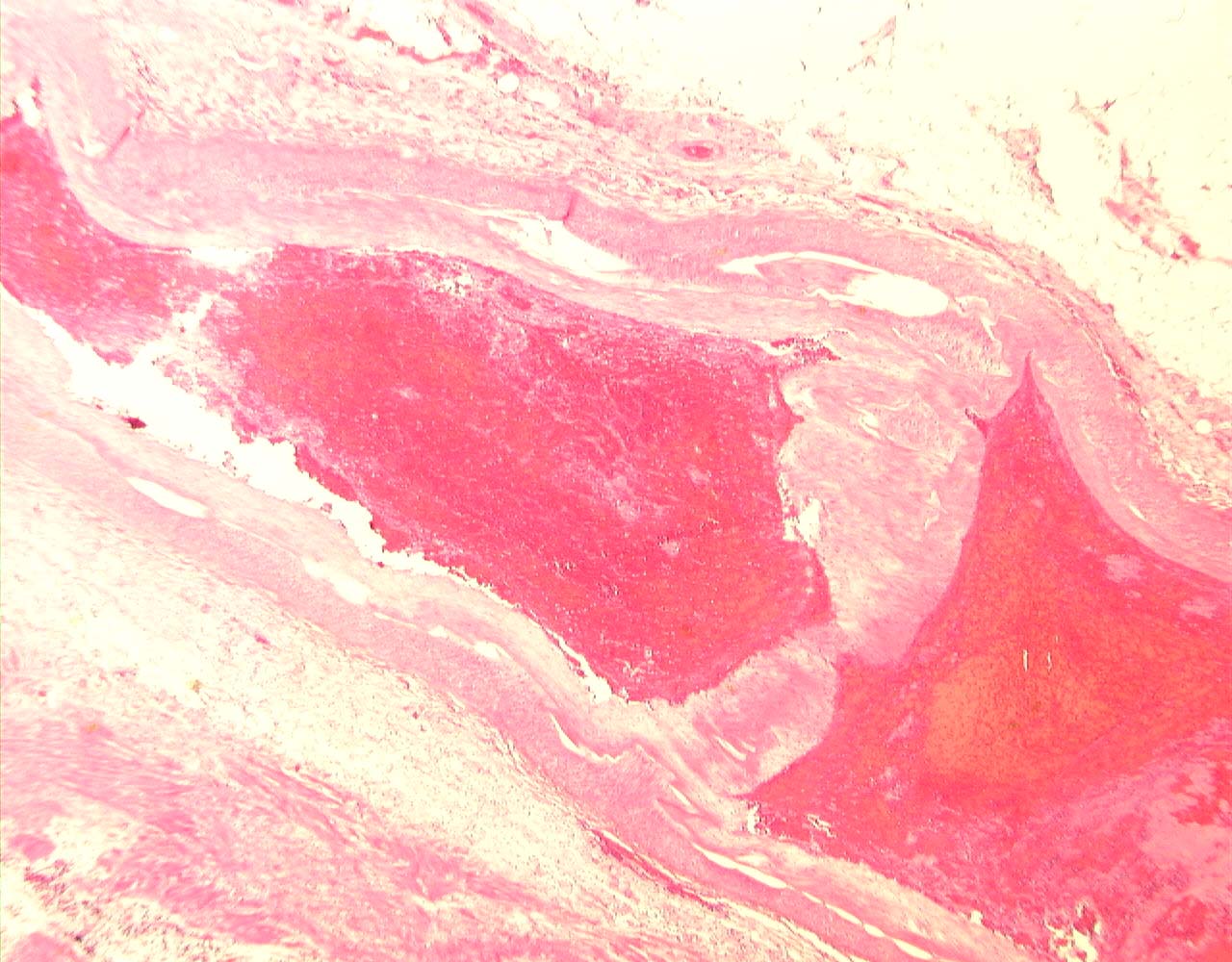
The kidney, on slicing, showed diffuse cortical pallor and multifocal paler cortical areas. The main renal artery appeared thrombosed.
(To View Original Images Click on Thumbnail)
 |
 |
 |
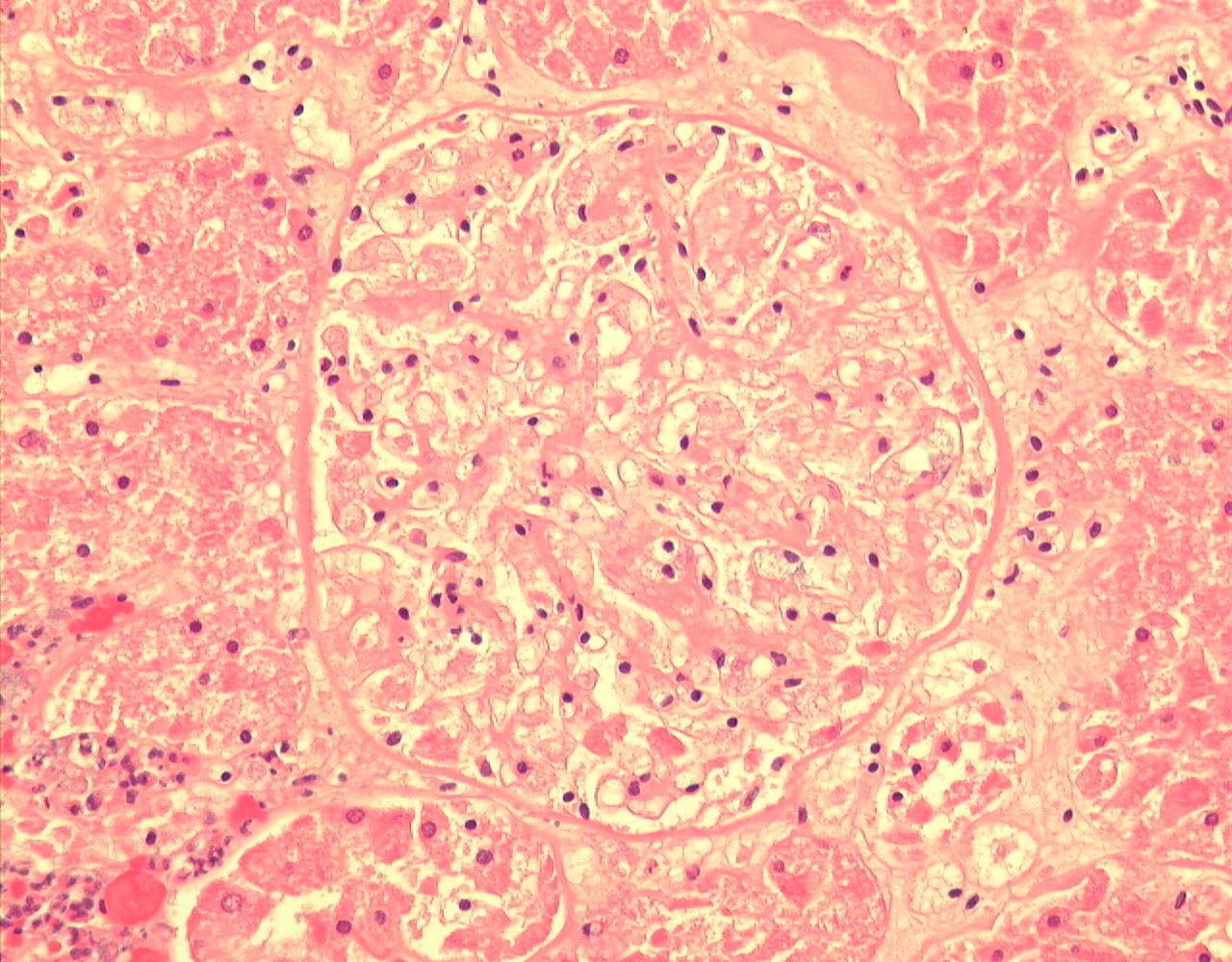
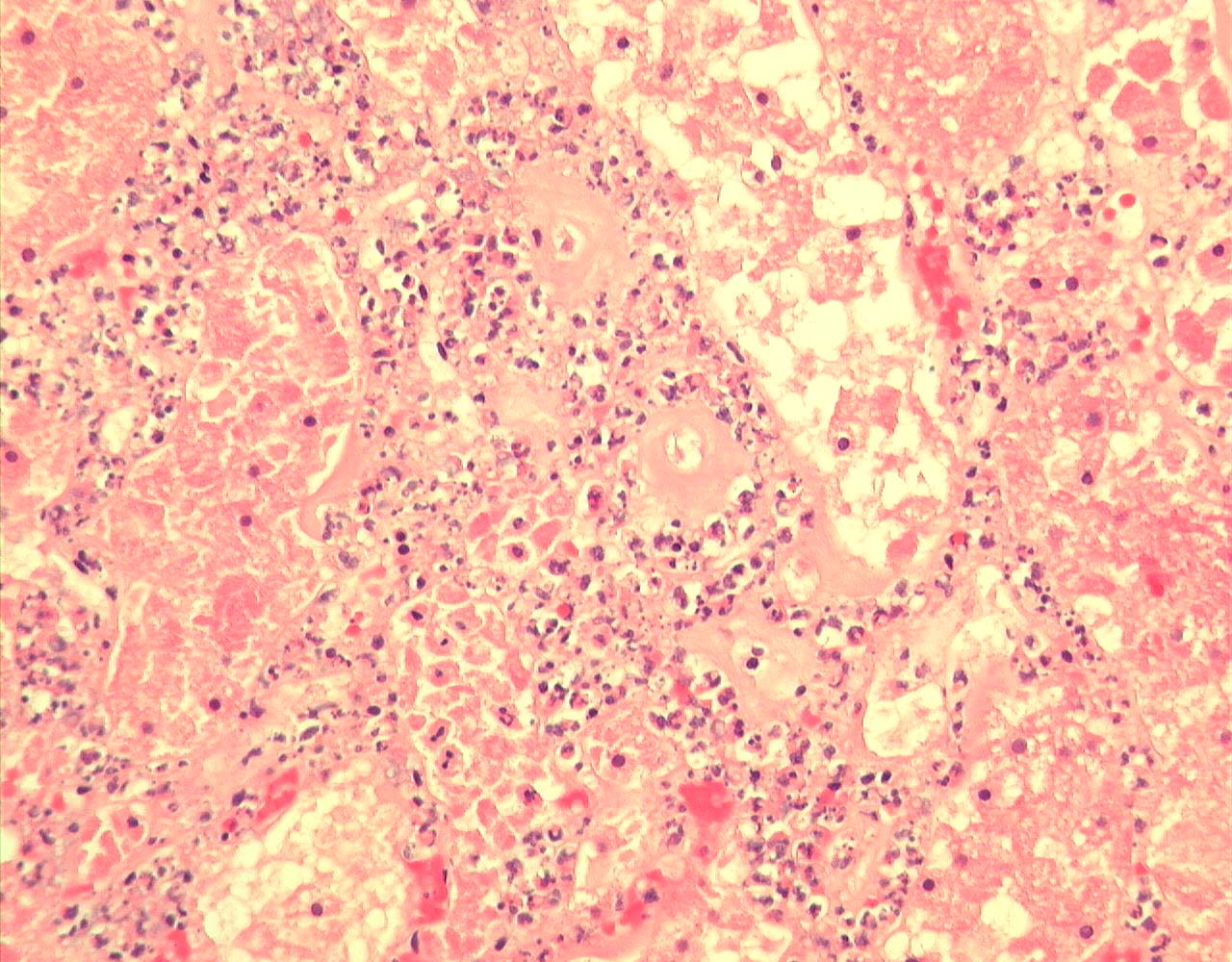
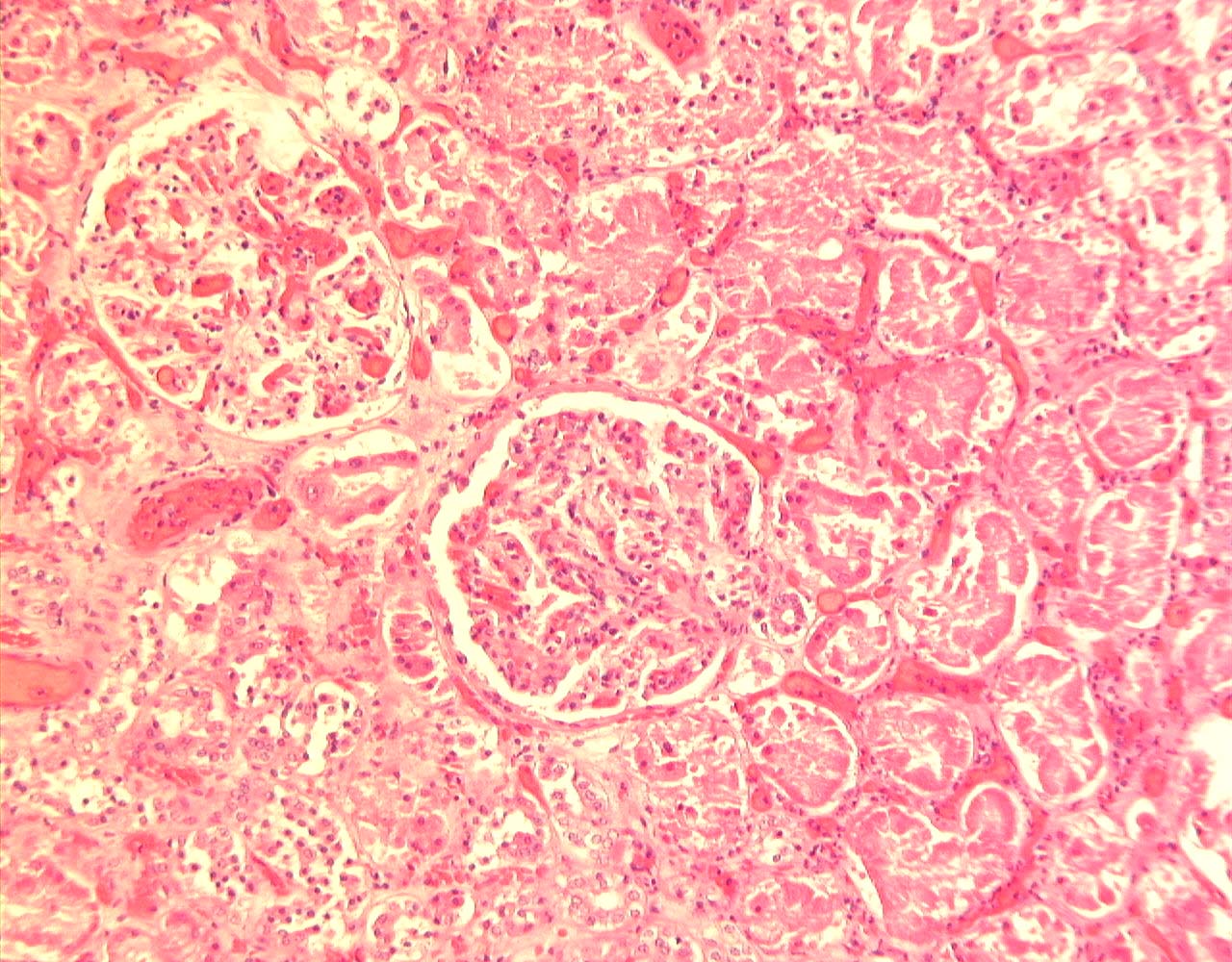
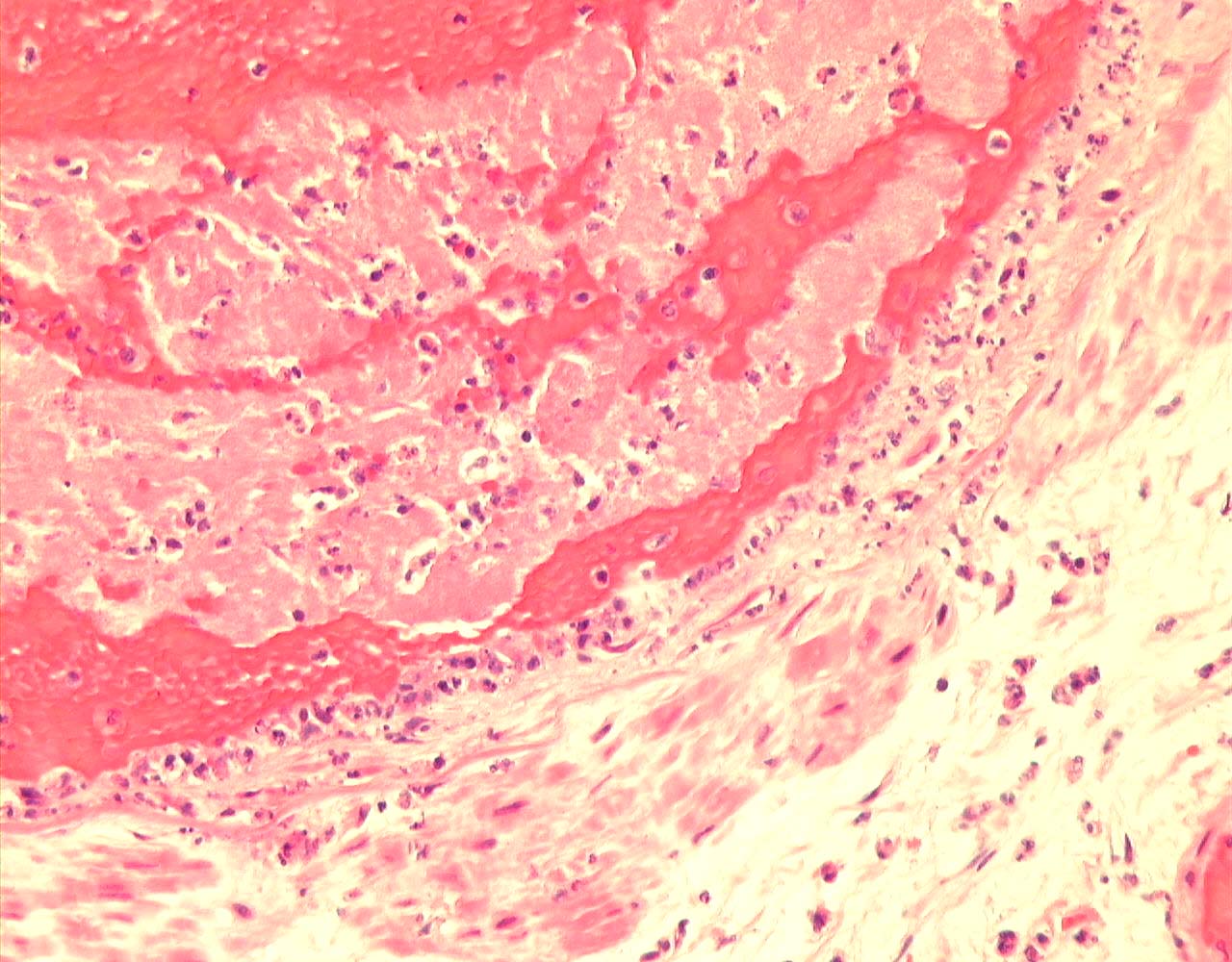
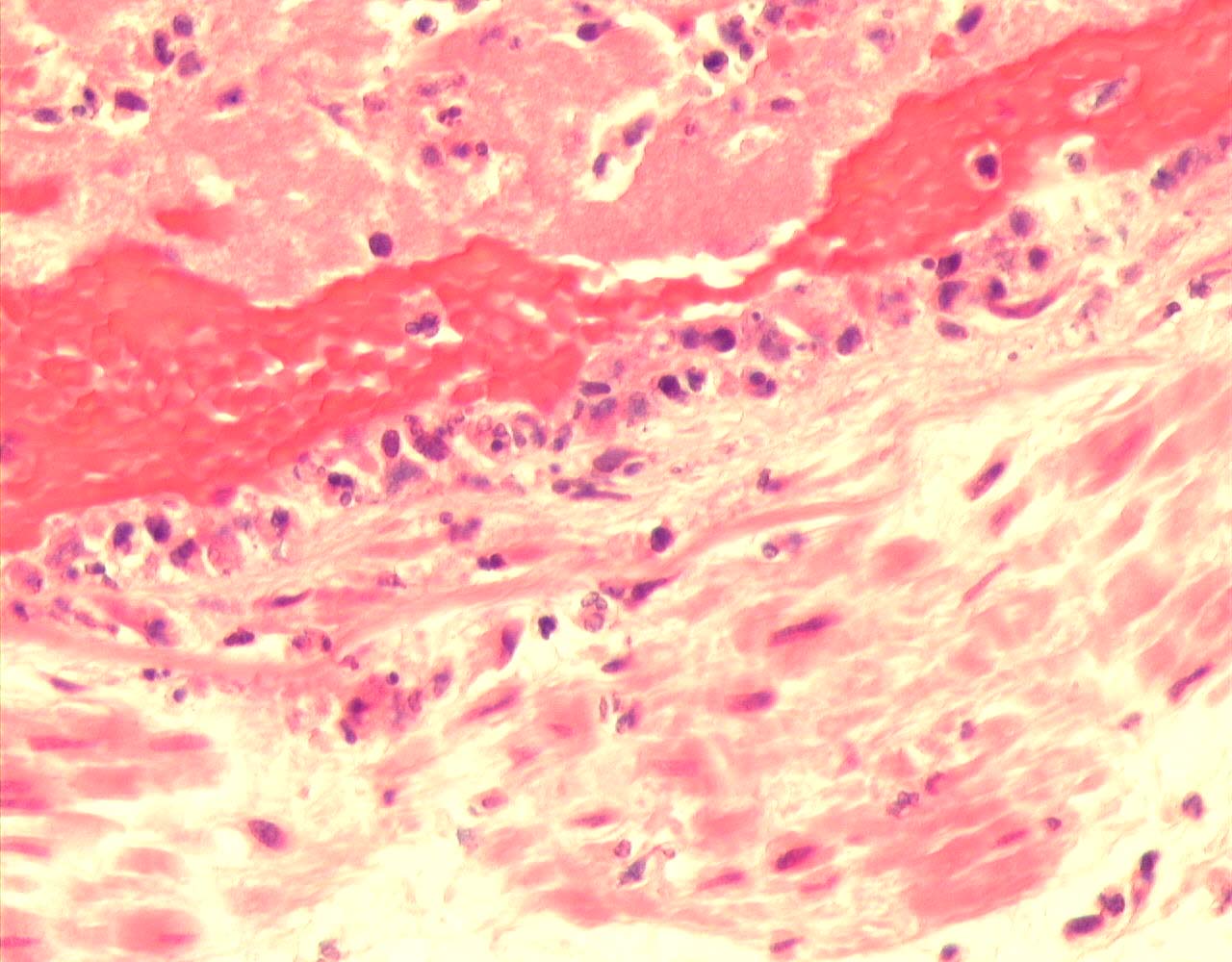
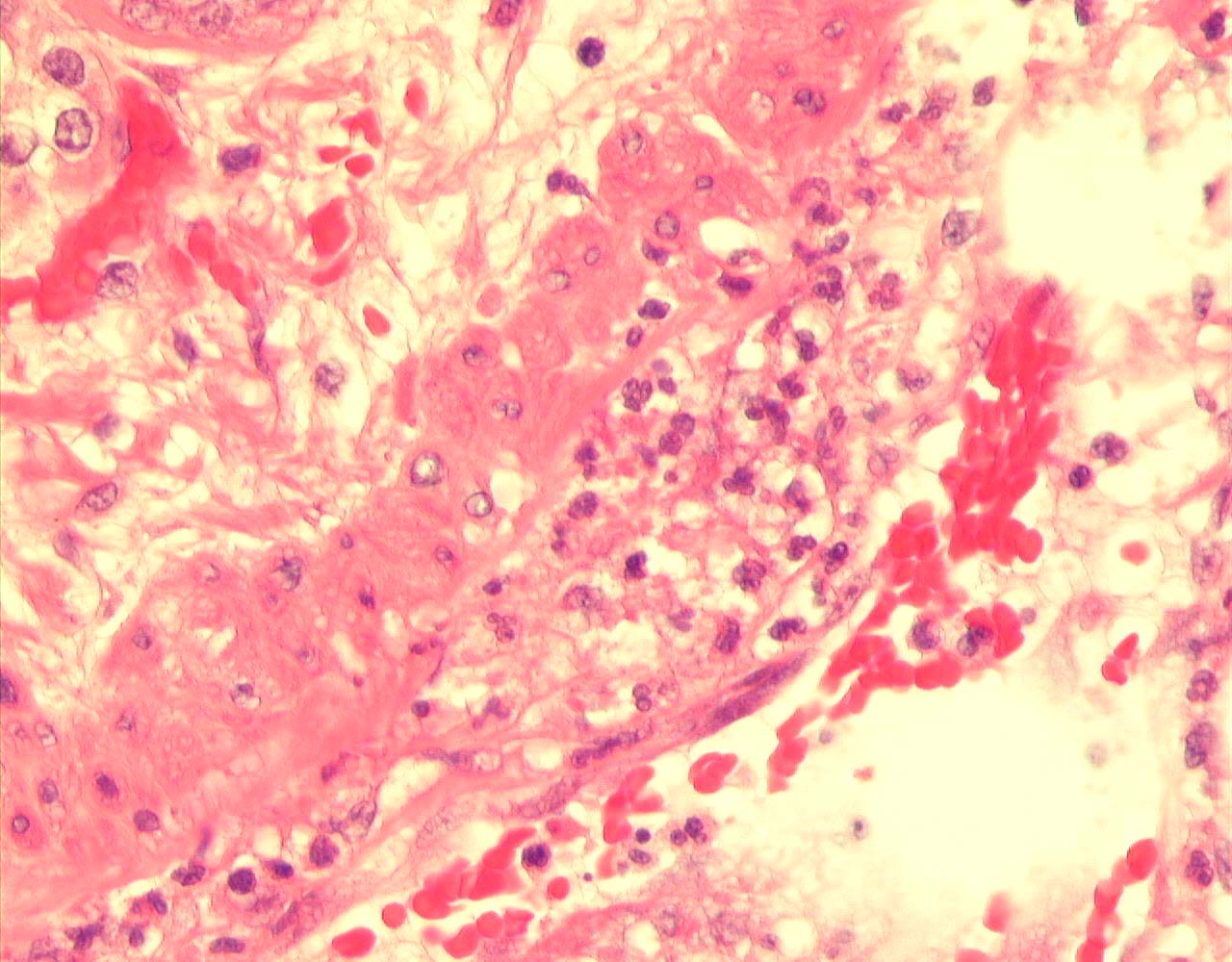
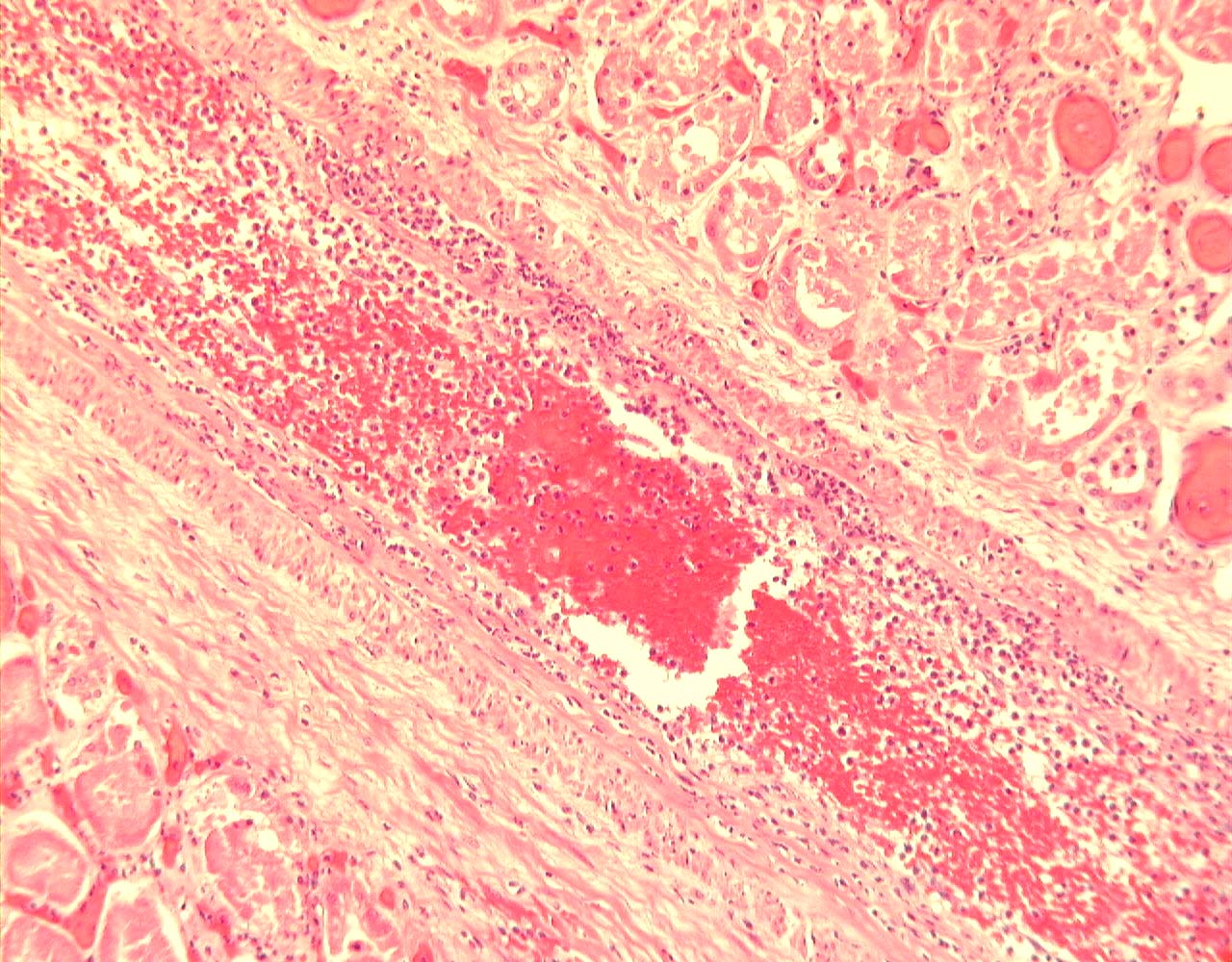
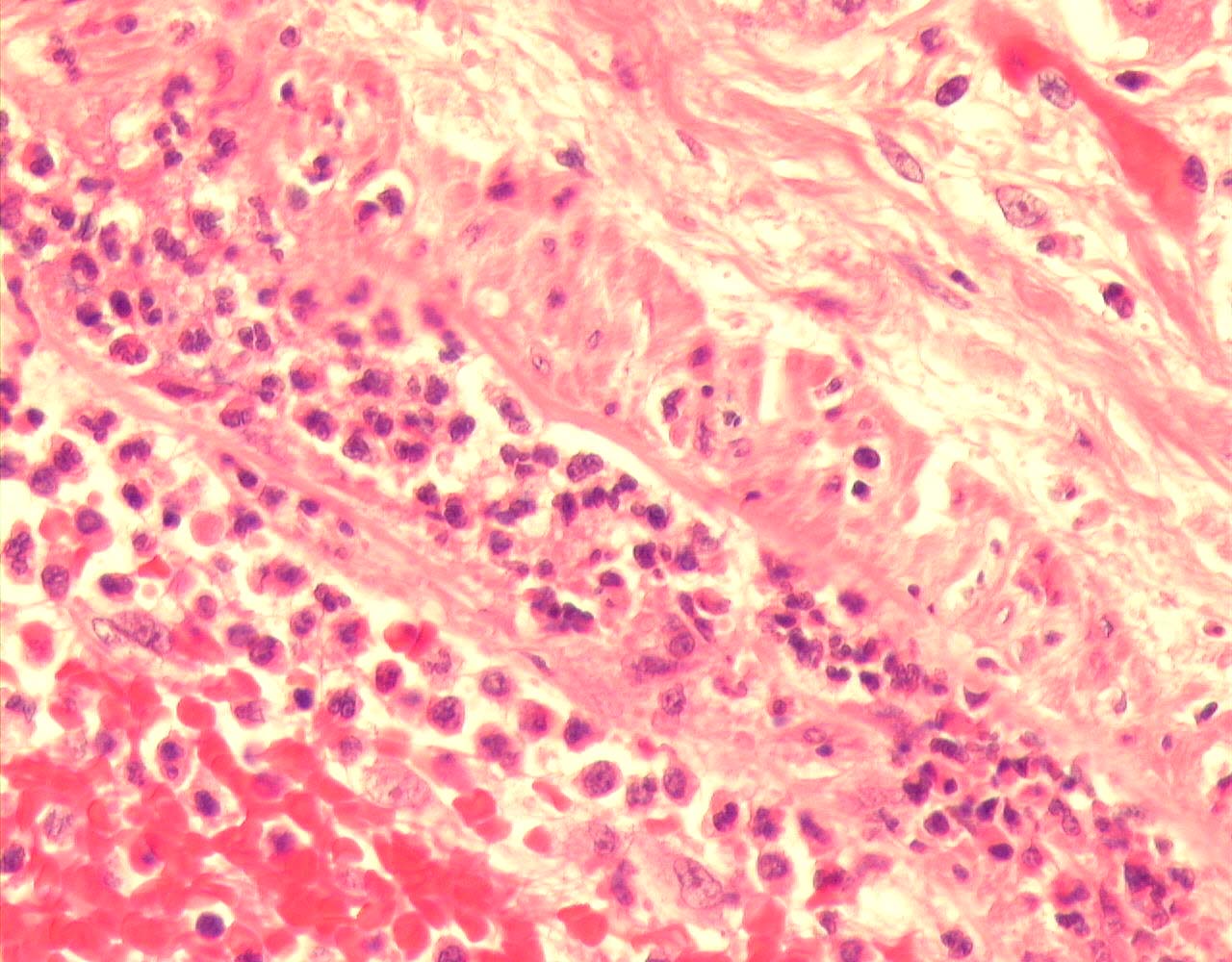
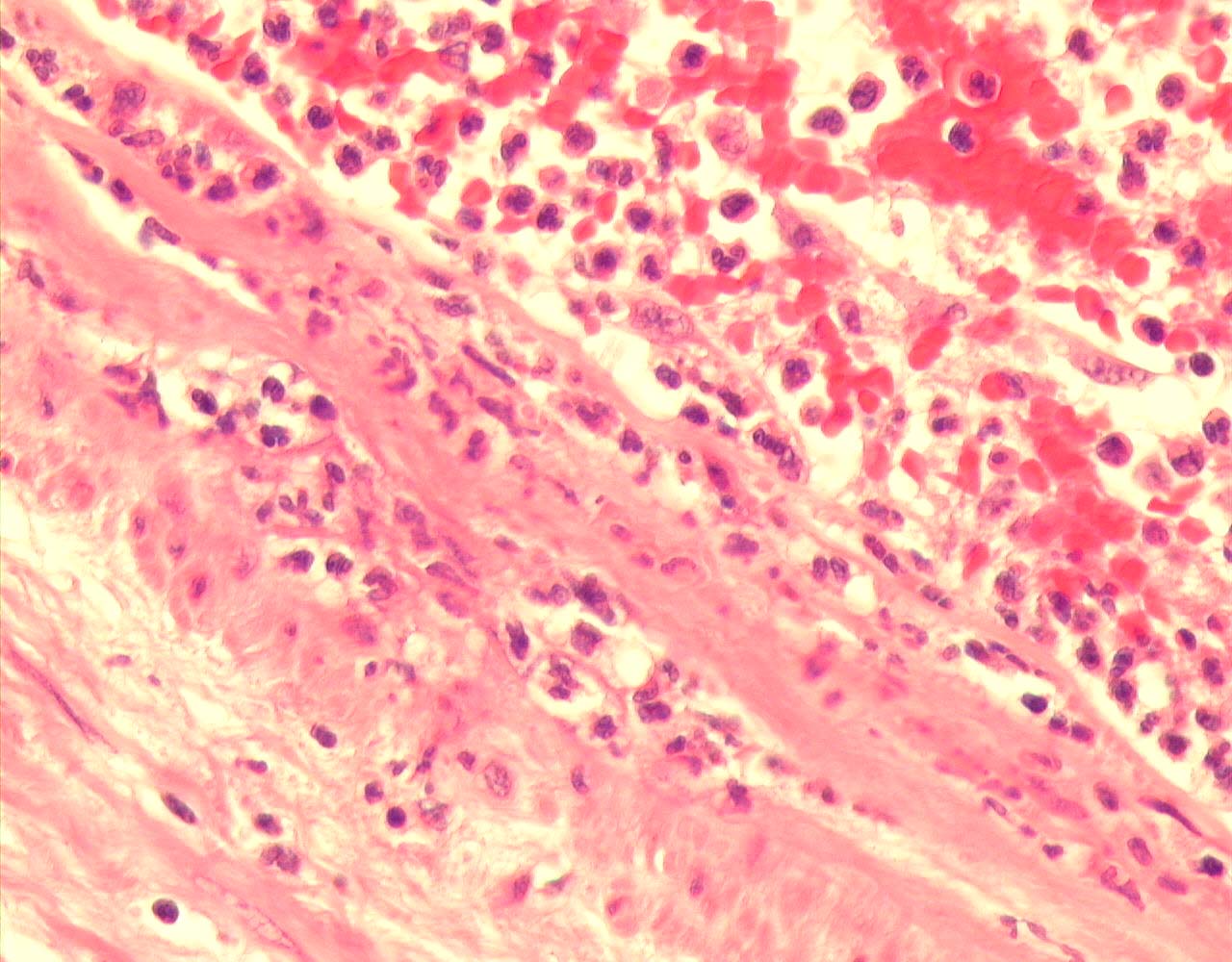
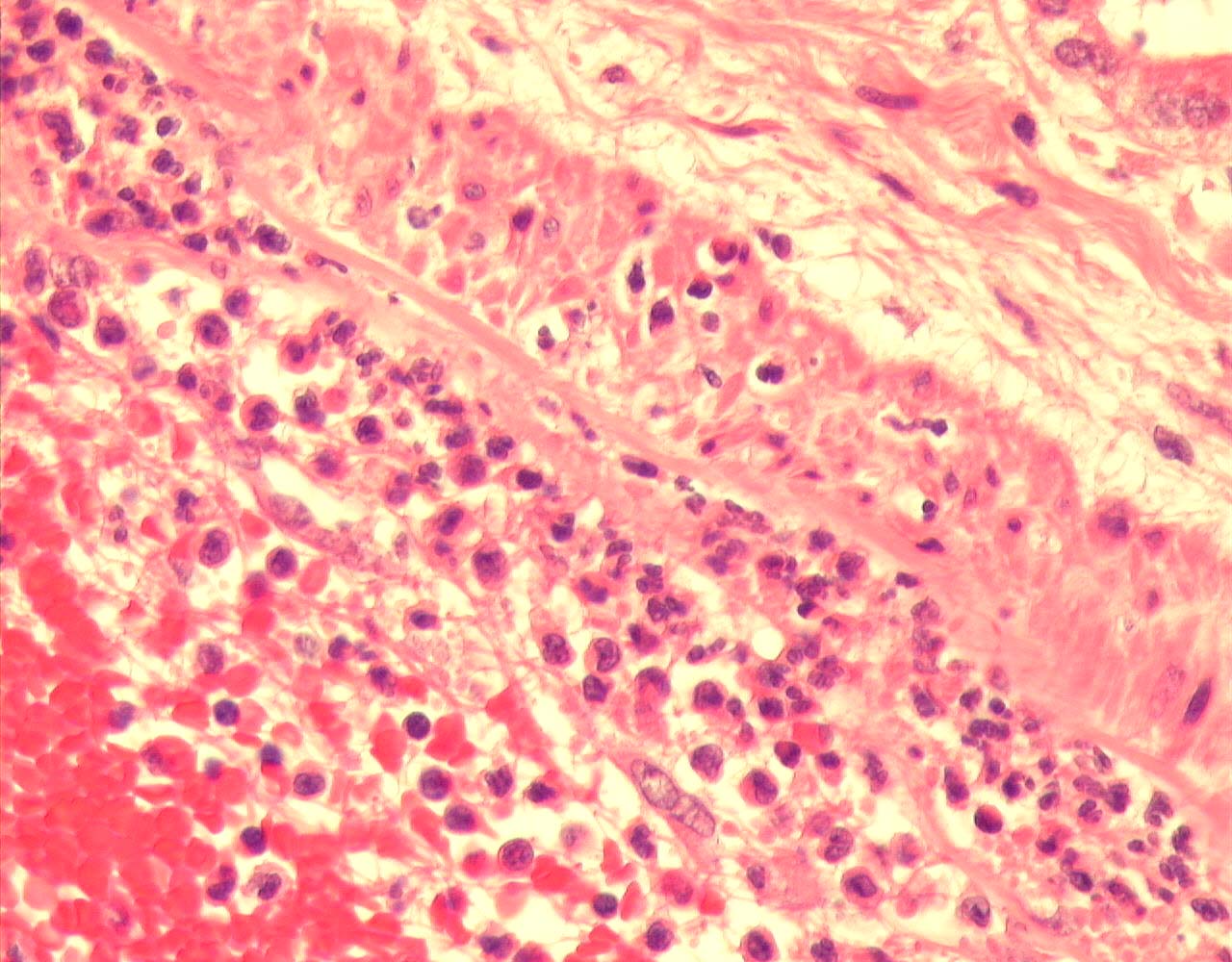
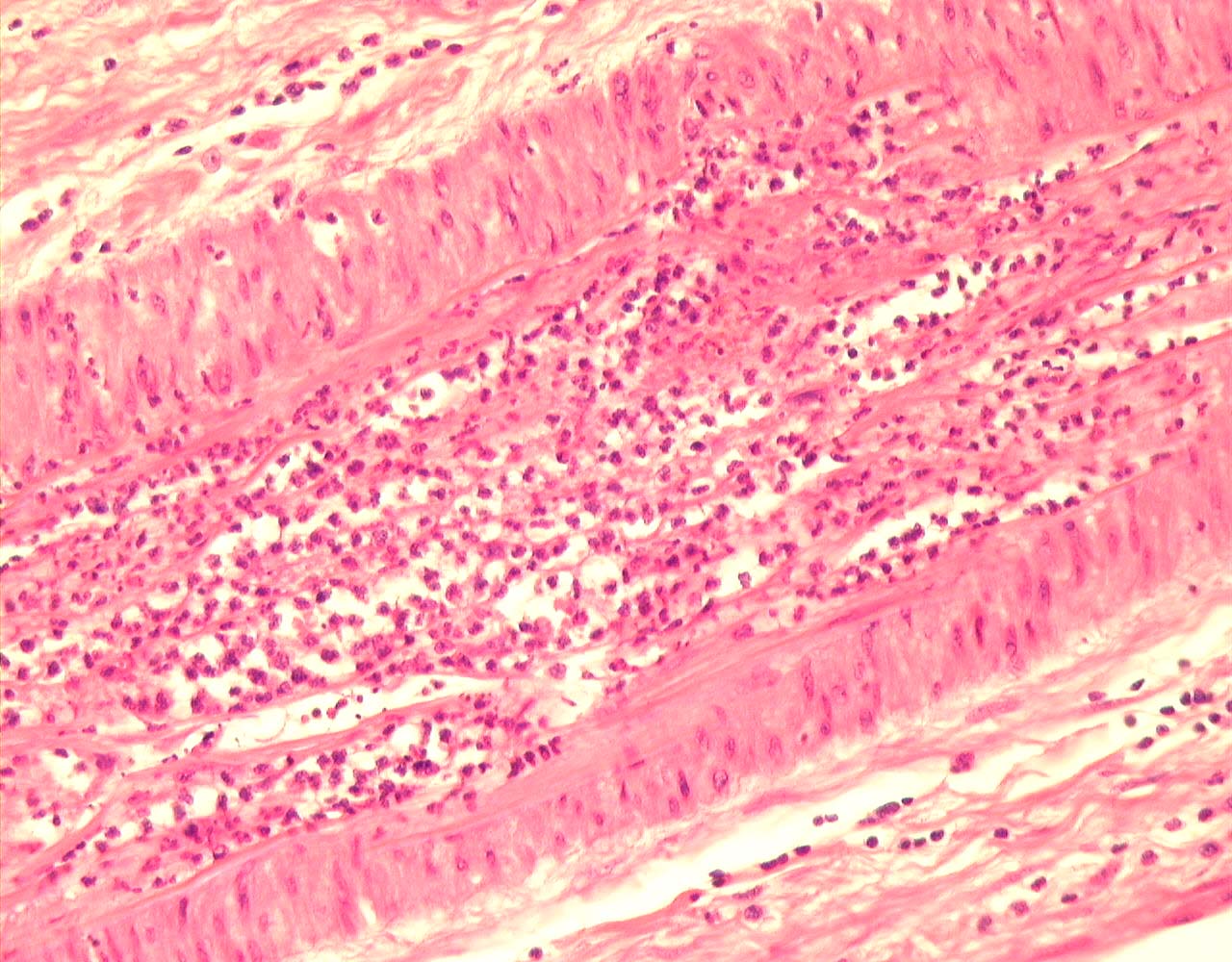
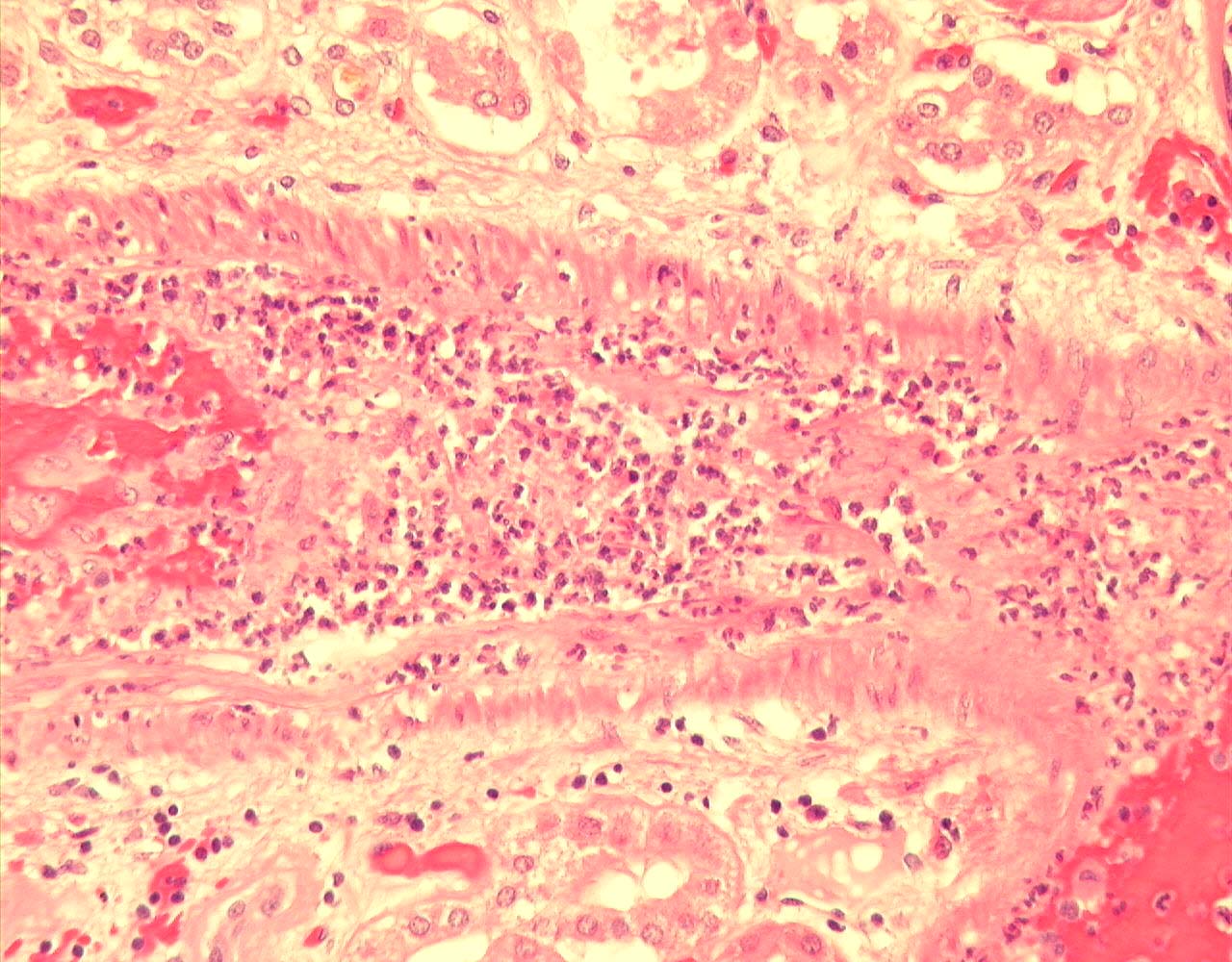
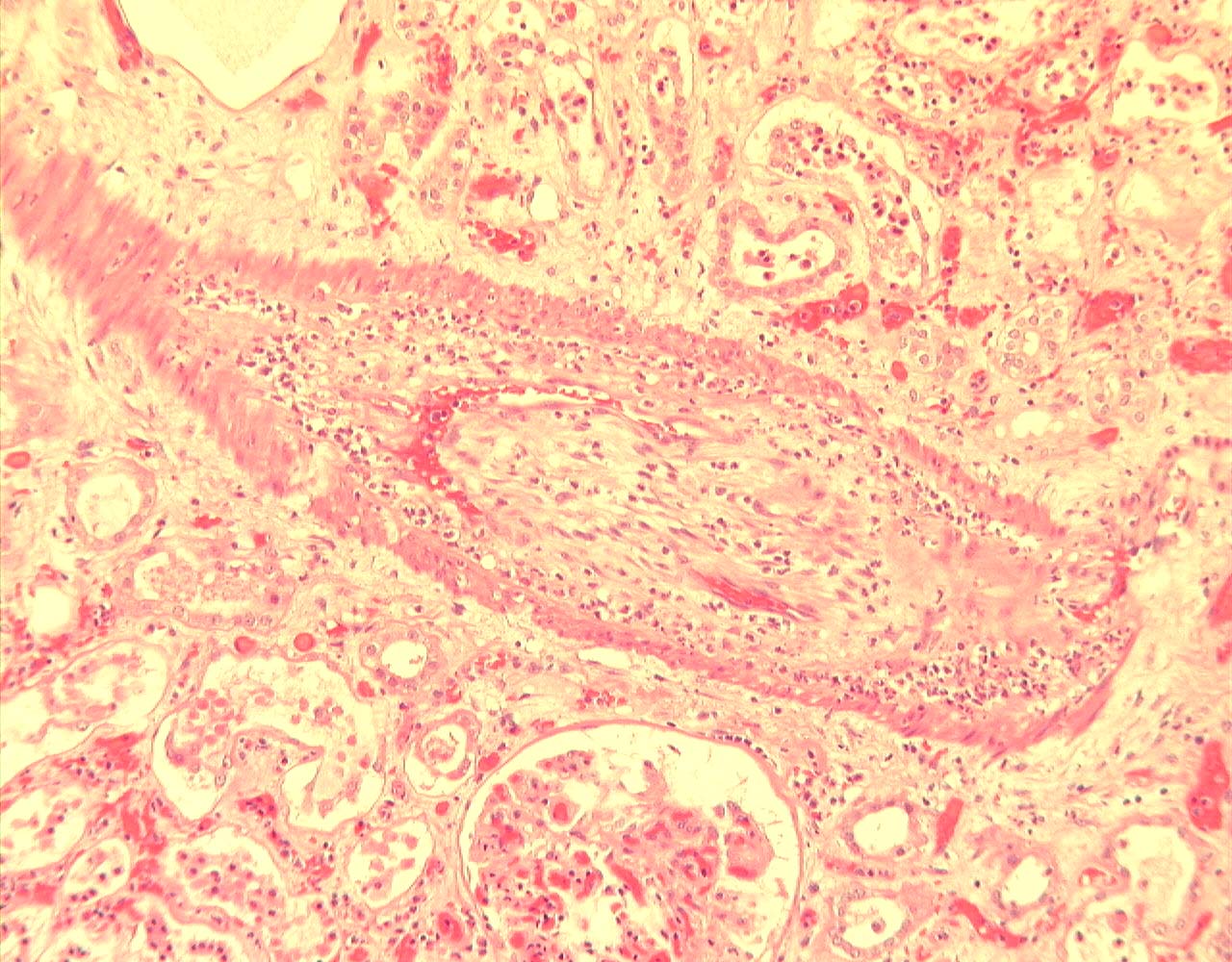
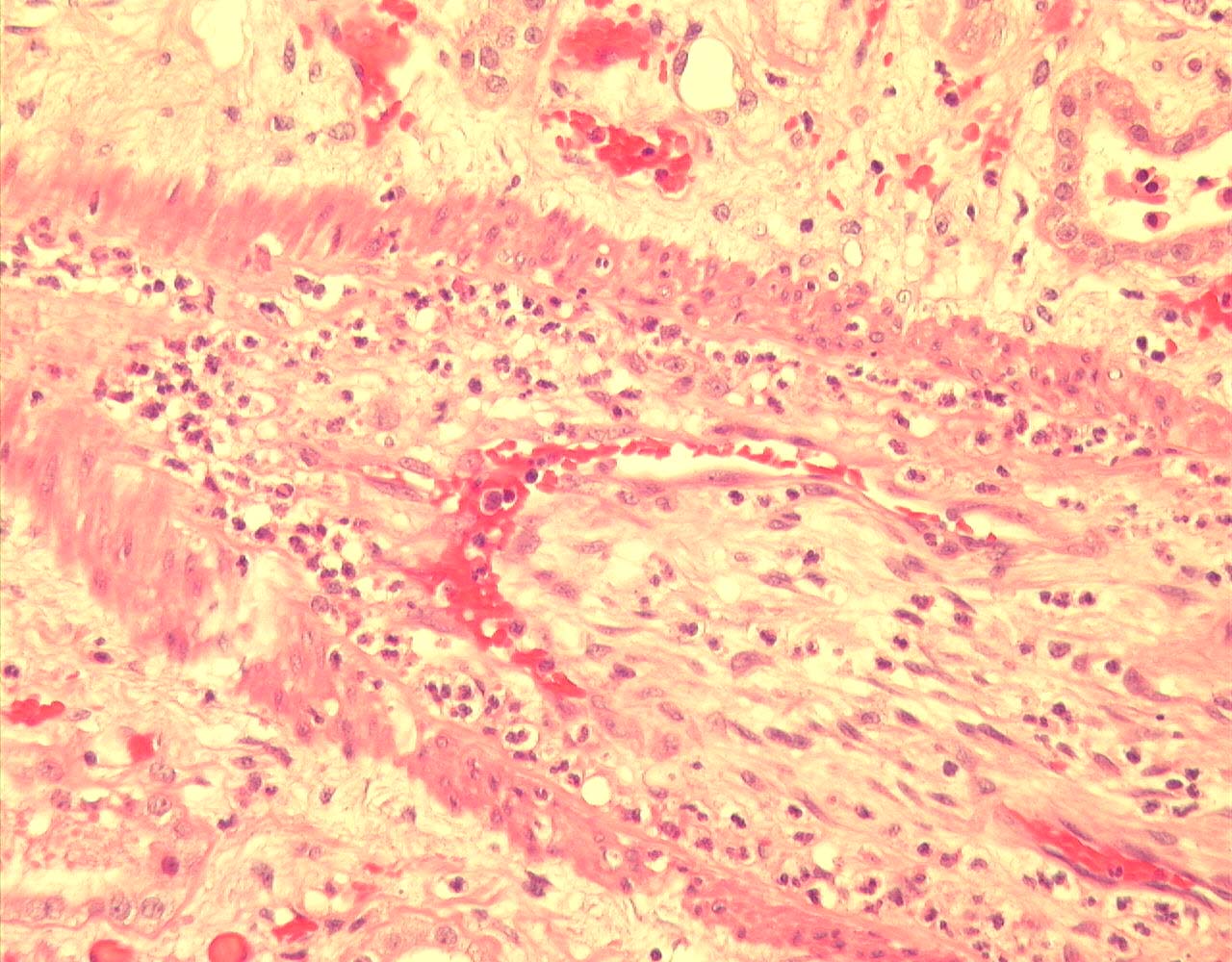
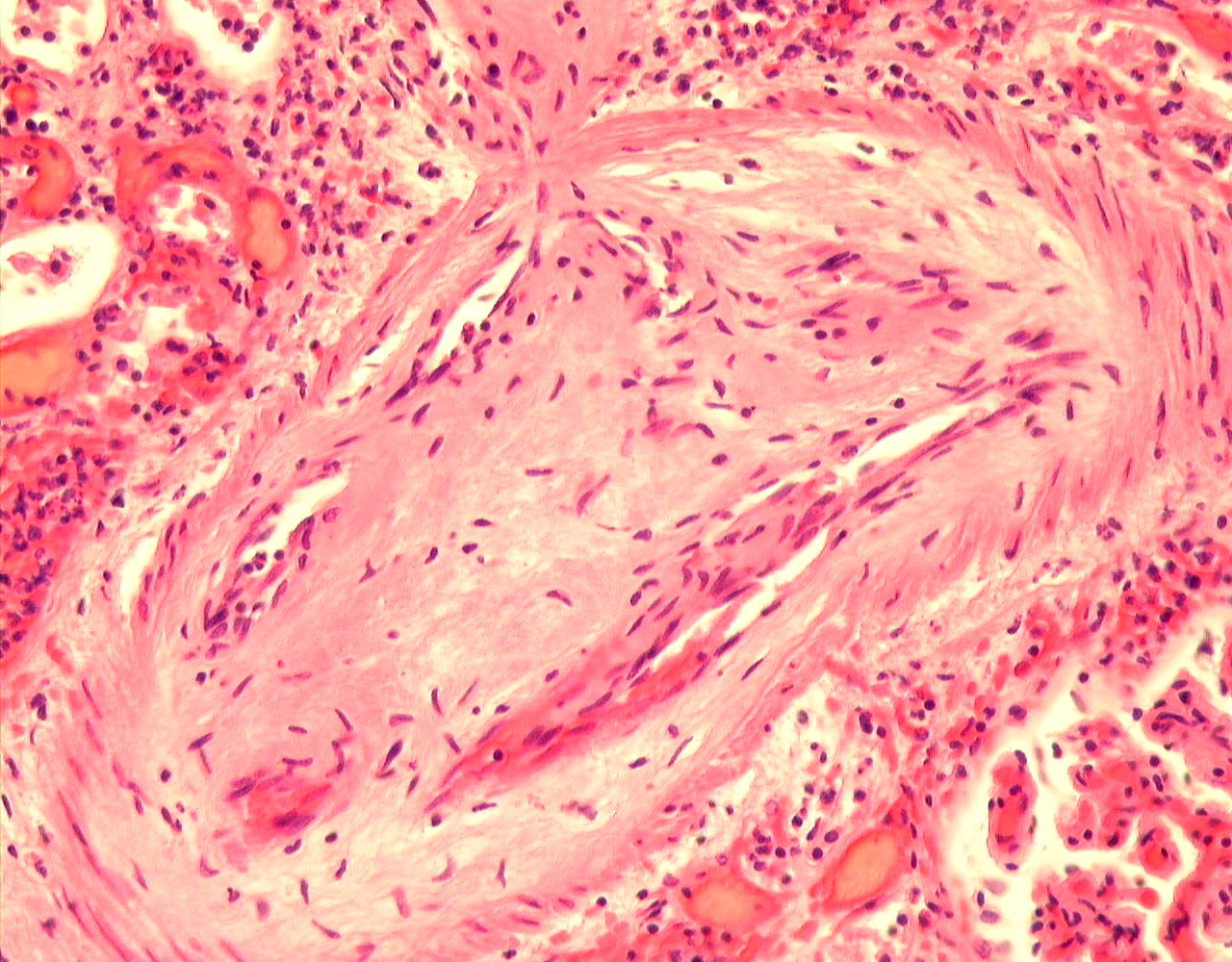
On microscopy, multifocal areas of cortical infarction with an interstitial neutrophil polymorph infiltrate at edge of infarcts.
 |
 |
 |
 |
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
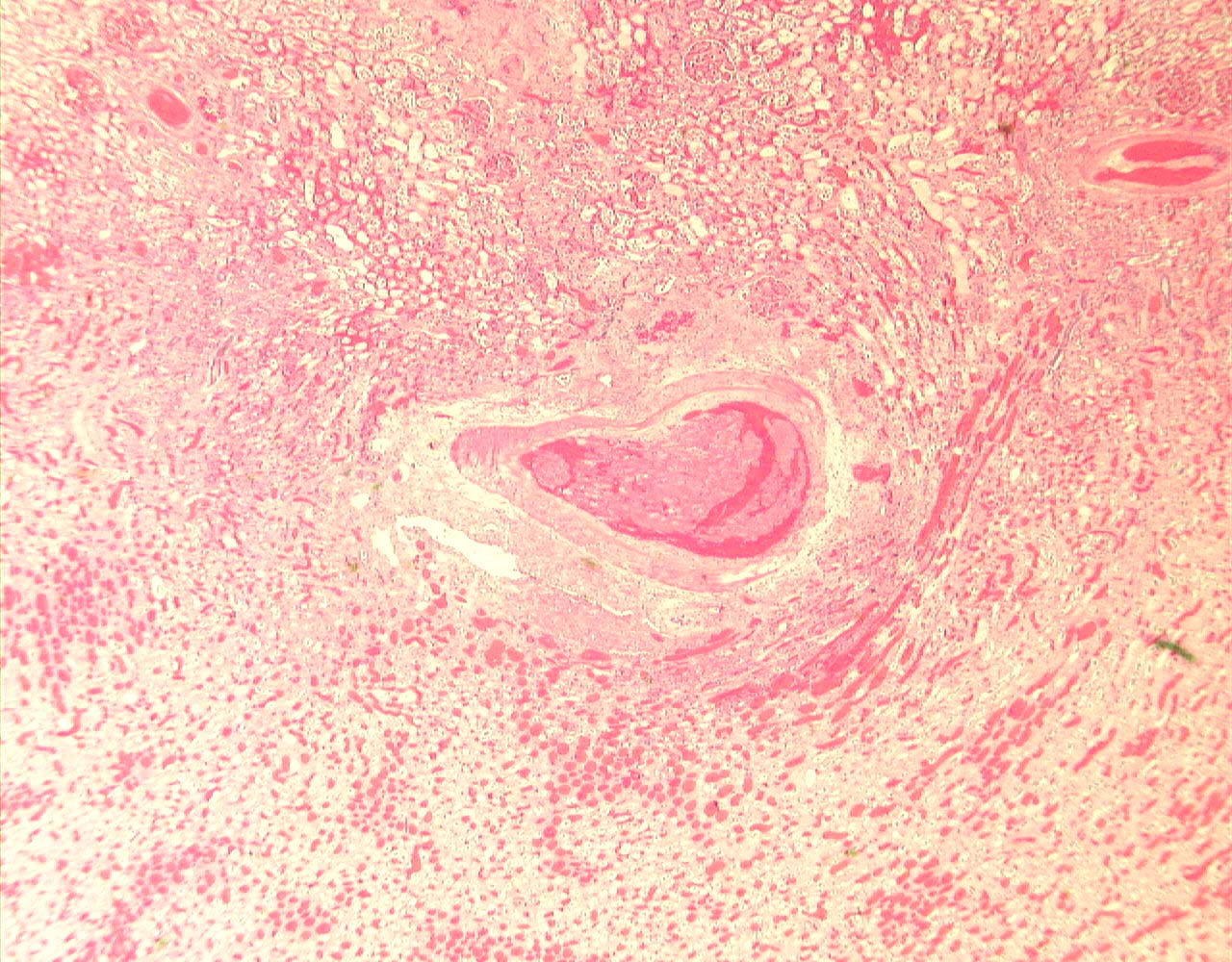
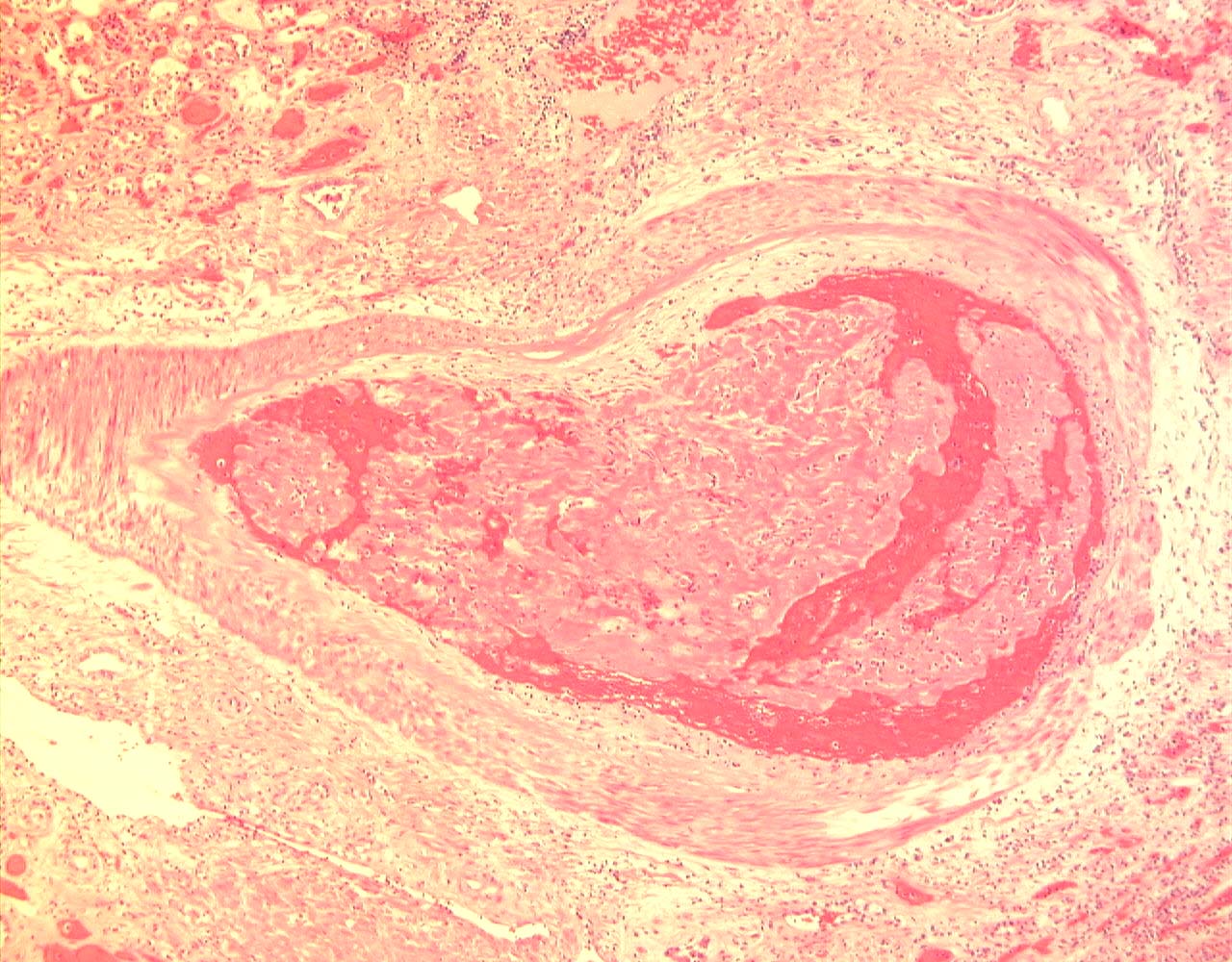
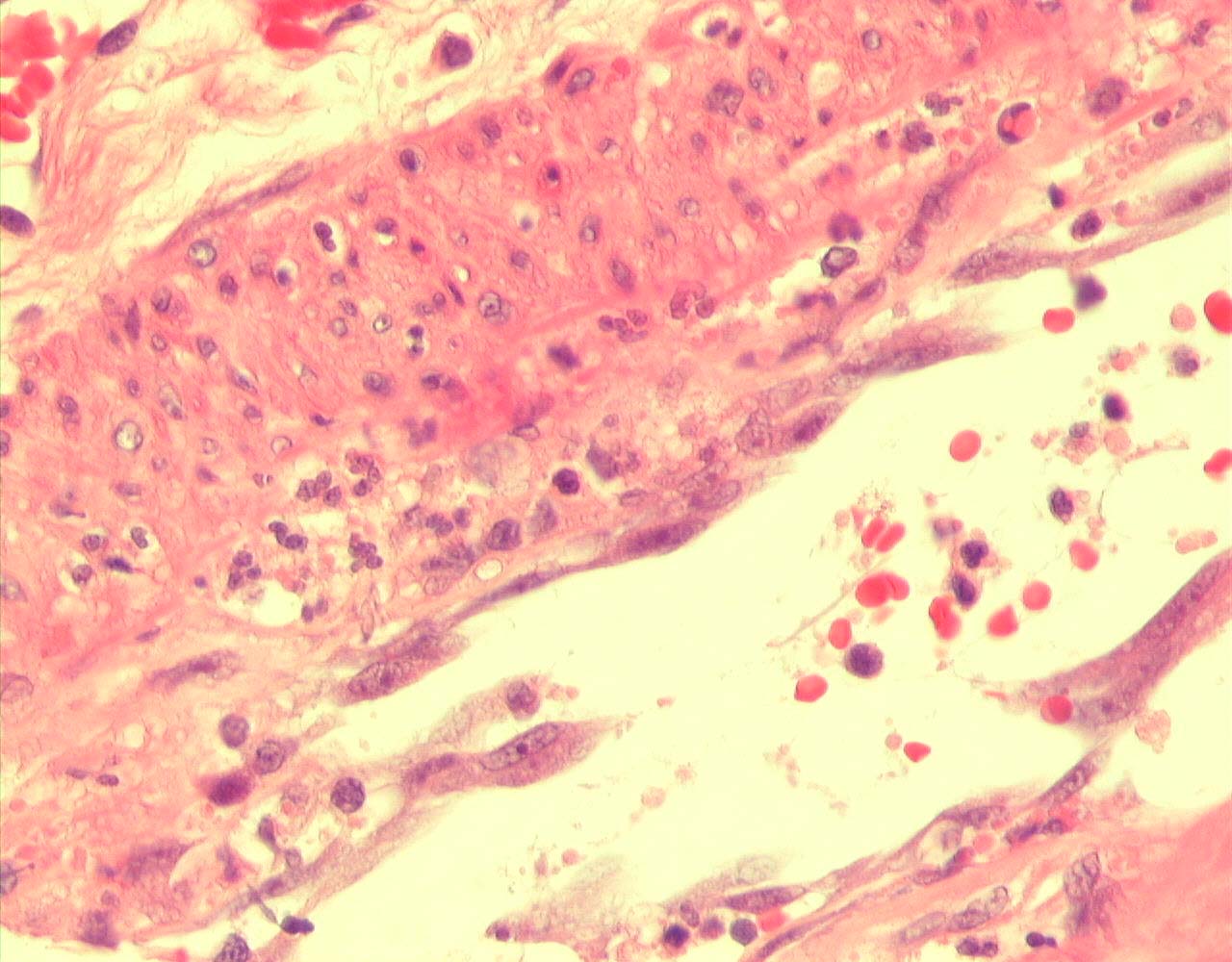
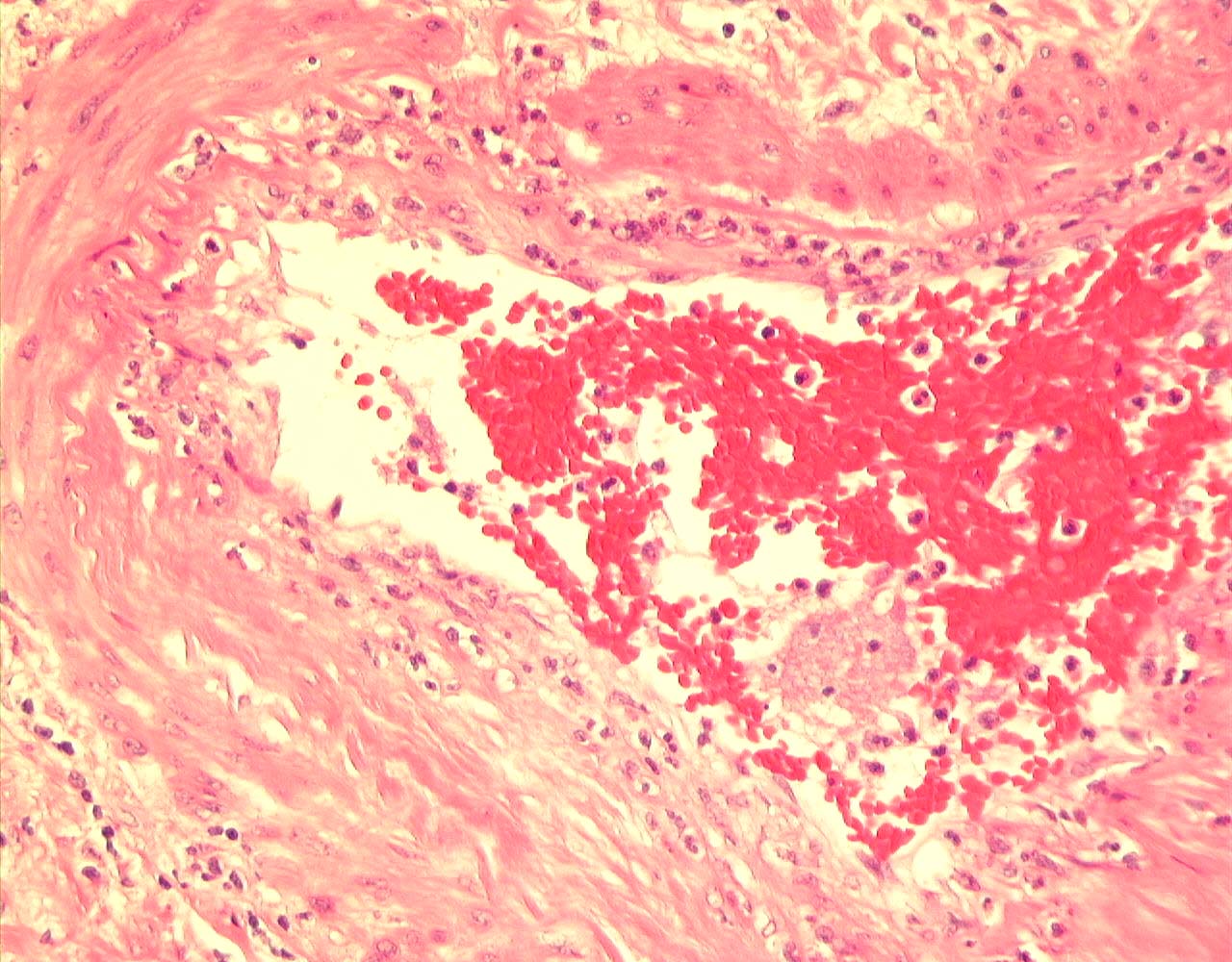
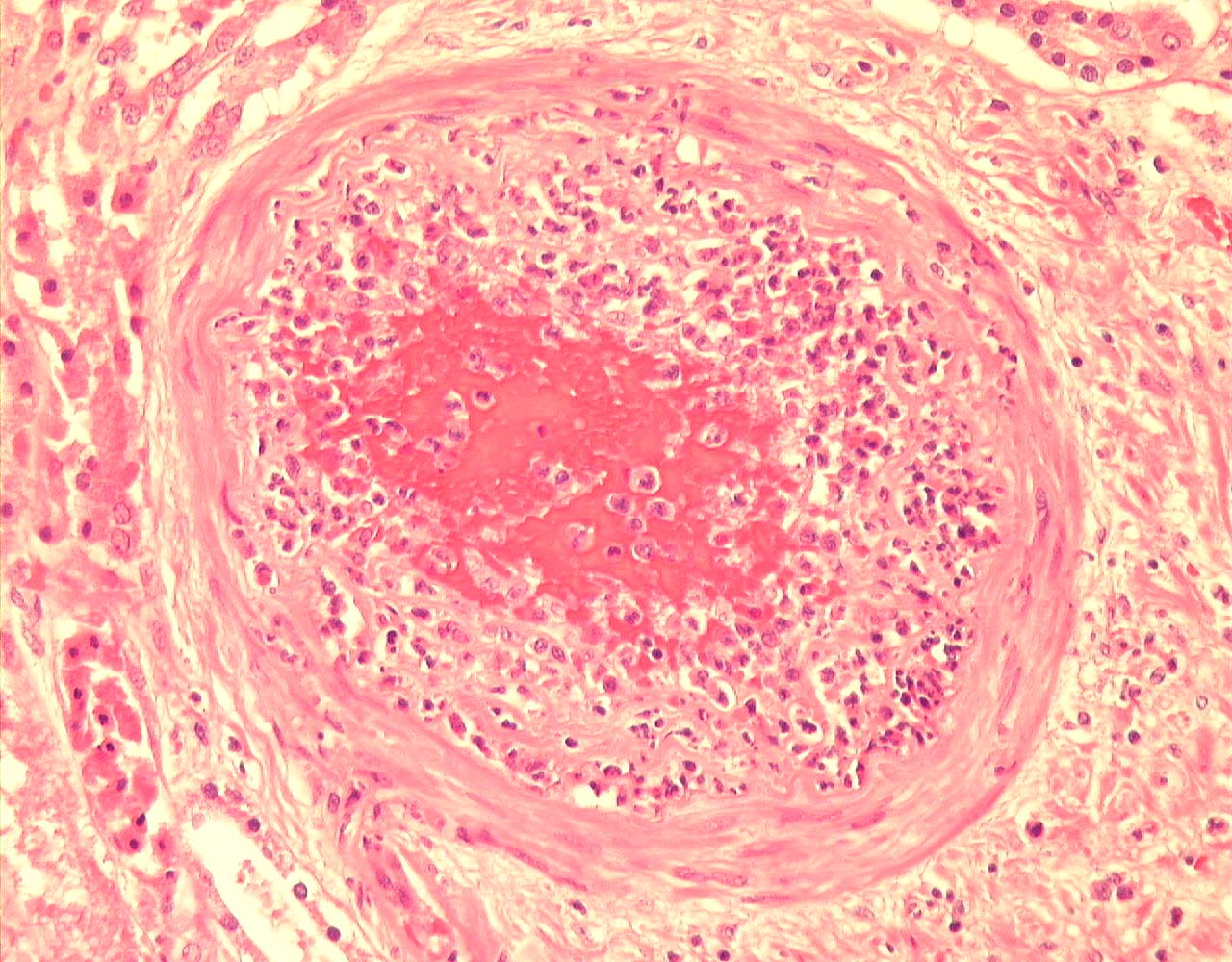
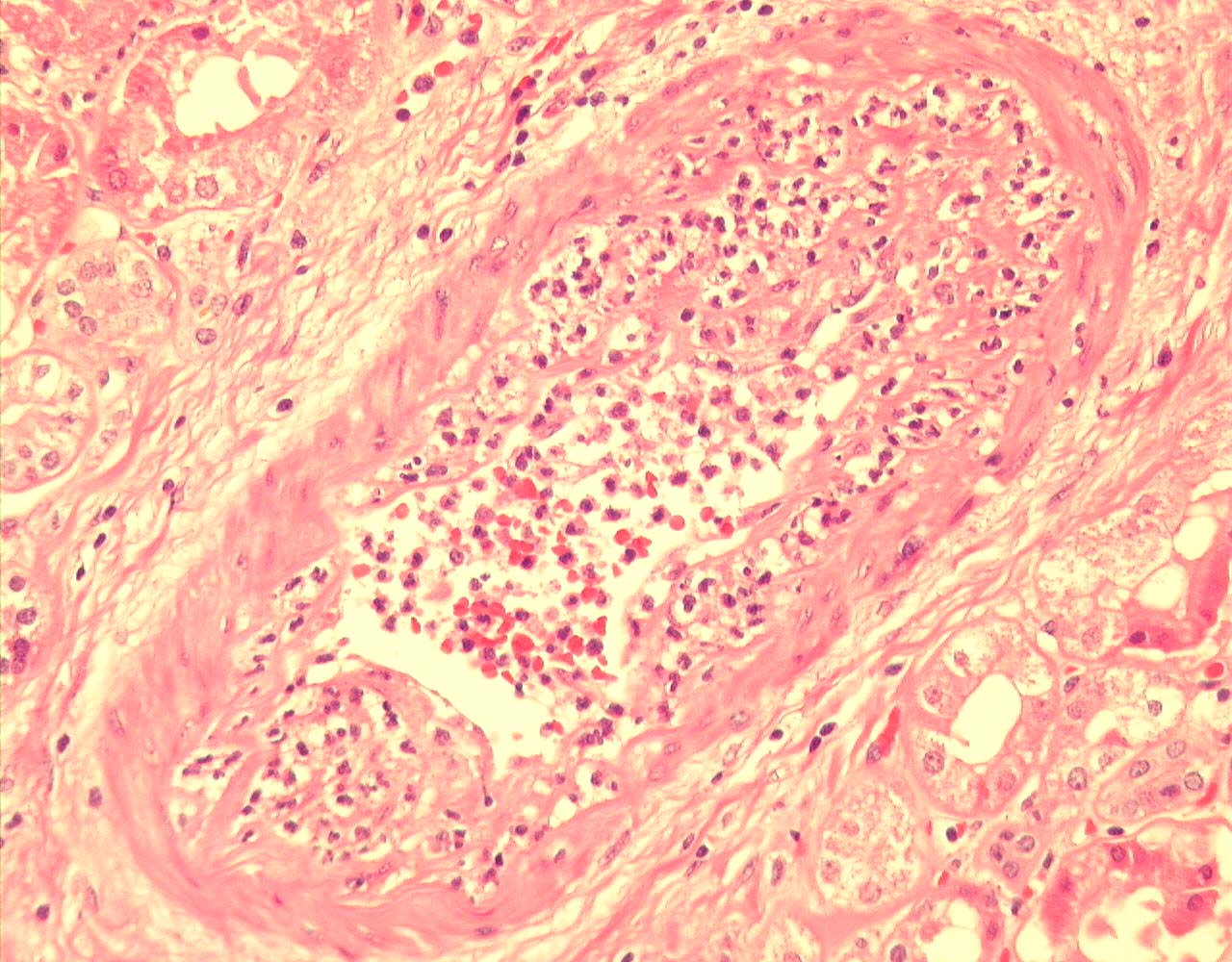
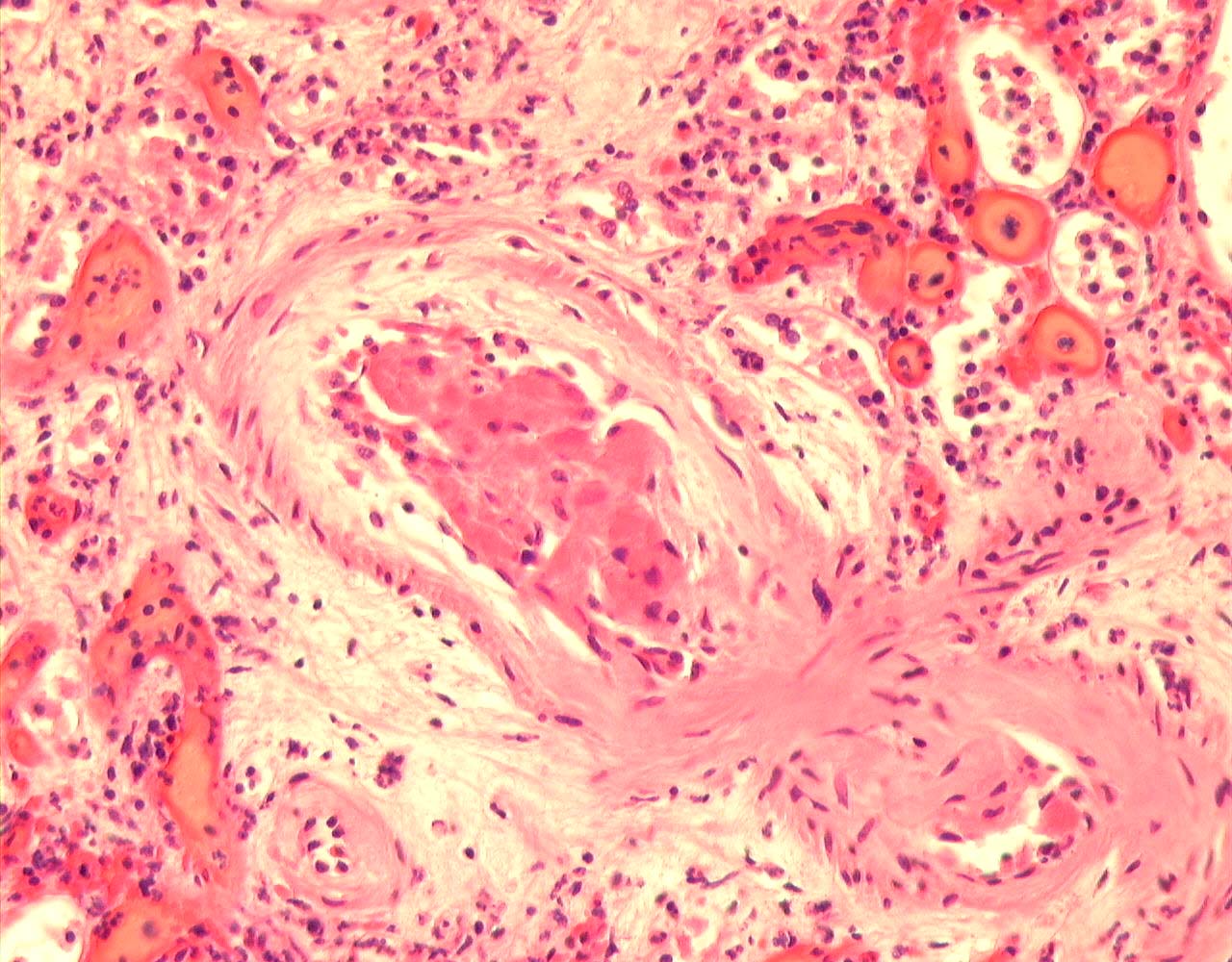
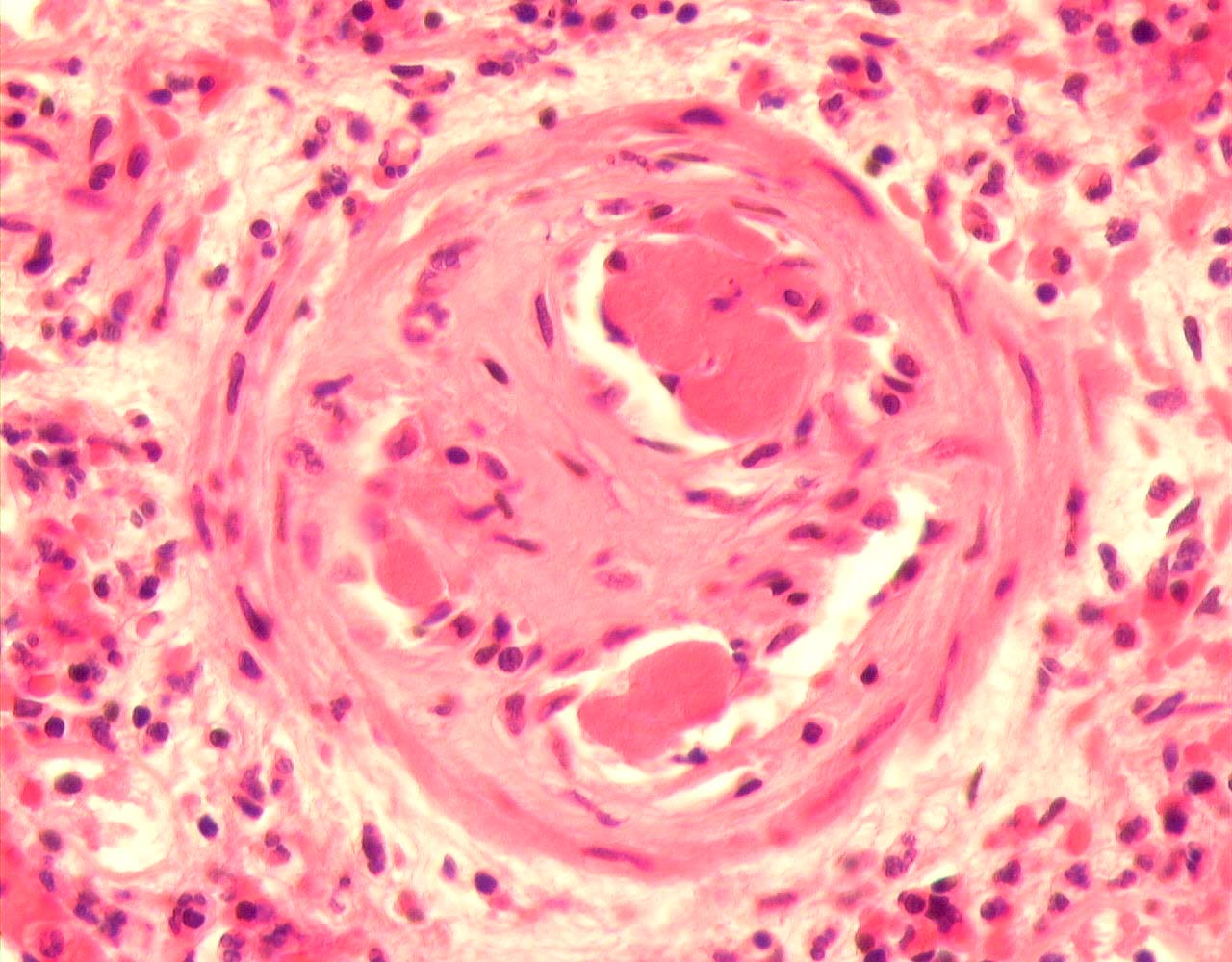
In summary, there is multifocal cortical infarction, arterial thromboses, a polymorph-rich non-necrotising arteritis, ATN and mild chronic allograft nephropathy.
Banff scores: g0,i1,t0,v3,ah0,cg0,mm0,ci1,ct1,cv1
PowerPoint Presentation
| Copyright � 2000-2007 cyberNephrologyTM
All rights reserved. Last Modified: Thursday March 08, 2007 05:21:15 PM |
[email protected] |